Overview
 Morton’s neuroma is a painful condition that affects the ball of your foot, most commonly the area between your third and fourth toes. Morton’s neuroma may feel as if you are standing on a pebble in your shoe or on a fold in your sock. Morton’s neuroma involves a thickening of the tissue around one of the nerves leading to your toes. This can cause a sharp, burning pain in the ball of your foot. Your toes also may sting, burn or feel numb. High-heeled shoes have been linked to the development of Morton’s neuroma. Many people experience relief by switching to lower heeled shoes with wider toe boxes. Sometimes corticosteroid injections or surgery may be necessary.
Morton’s neuroma is a painful condition that affects the ball of your foot, most commonly the area between your third and fourth toes. Morton’s neuroma may feel as if you are standing on a pebble in your shoe or on a fold in your sock. Morton’s neuroma involves a thickening of the tissue around one of the nerves leading to your toes. This can cause a sharp, burning pain in the ball of your foot. Your toes also may sting, burn or feel numb. High-heeled shoes have been linked to the development of Morton’s neuroma. Many people experience relief by switching to lower heeled shoes with wider toe boxes. Sometimes corticosteroid injections or surgery may be necessary.
Causes
Morton’s neuroma is an inflammation caused by a buildup of fibrous tissue on the outer coating of nerves. This fibrous buildup is a reaction to the irritation resulting from nearby bones and ligaments rubbing against the nerves. Irritation can be caused by Wearing shoes that are too tight. Wearing shoes that place the foot in an awkward position, such as high heels. A foot that is mechanically unstable. Repetitive trauma to the foot such as from sports activities like tennis, basketball, and running. Trauma to the foot caused by an injury such as a sprain or fracture. It is unusual for more than one Morton’s neuroma to occur on one foot at the same time. It is rare for Morton’s neuroma to occur on both feet at the same time.
Symptoms
Many patients describe the sensation as a burning pain in the ball of the foot that often radiates to the toes. Initially, the pain may become much more apparent when the person wears tight, narrow or high-heeled shoes, or engages in activities which place pressure on the foot. Eventually, symptoms may be continuous and last for days, and even weeks. MRI (magnetic resonance imaging) scans have revealed Morton’s neuroma lesions in patients who had no symptoms at all. Symptoms can become so disrupting that many affected individuals become anxious about walking, or even placing their foot on the ground.
Diagnosis
A doctor can usually identify Morton’s neuroma during a physical exam. He or she will squeeze or press on the bottom of your foot or squeeze your toes together to see if it hurts. Your doctor may also order an X-ray of your foot to make sure nothing else is causing the pain.
Non Surgical Treatment
Treatment for Morton?s neuroma will depend on how long you’ve had the condition and its severity. Simple non-surgical treatments are effective for some people. Others may need surgery. If Morton’s neuroma is diagnosed early, treatment will aim to reduce the pressure on the affected nerve. This is usually the nerve between the third and fourth toe bones (metatarsals). Your GP or podiatrist (foot specialist) may recommend changing the type of shoes you usually wear, shoes with a wider toe area may help ease the pressure on the nerve in your foot. Using orthotic devices, such as a support for the arch of your foot to help relieve the pressure on the nerve. Anti-inflammatory painkillers or a course of steroid injections into the affected area of your foot may help ease the pain and inflammation. Alcohol and local anaesthetic is injected into your foot using ultrasound for guidance, studies have shown that this type of treatment is effective. Resting your foot and massaging your toes may also help to relieve the pain. You can make an ice pack by freezing a small bottle of water and rolling it over the affected area.
Surgical Treatment
Surgical treatment has provided relief in some cases while poor results and surgical complications have resulted in other cases. It is believed that ligament weakness, as opposed to the pinching of nerves in the foot, may be to blame for recurrent pain in these situations. For reasons which are not fully understood, the incidence of Morton?s Neuroma is 8 to 10 times greater in women than in men.




 Overview
Overview Symptoms
Symptoms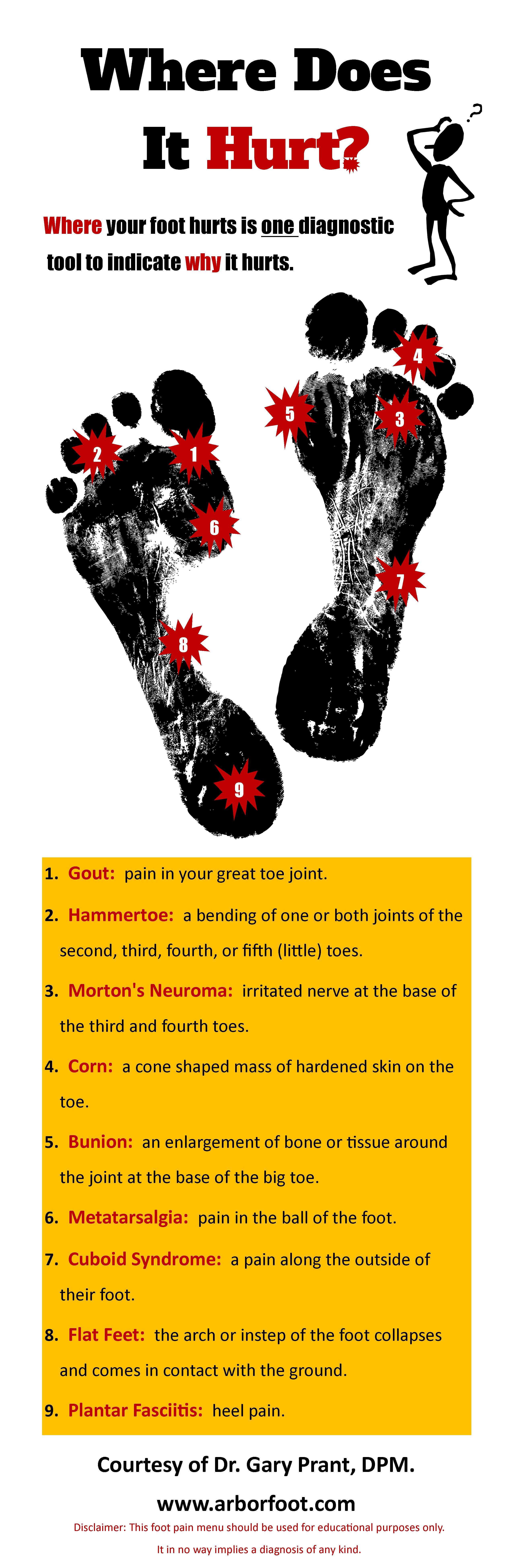 Prevention
Prevention Overview
Overview Symptoms
Symptoms





